脑部放疗,上午比下午敏感许多!+ X5 j$ V) x7 i- q7 Z
3 b D) Z) ^+ ]! t
" Z, A* U+ y) Z" ]) L" ]$ v& M
Cancer 2011 Jan 15;117(2):414-20. doi: 10.1002/cncr.25423. Epub 2010 Sep 9.& r" m9 G8 @' C8 ?- r
Gamma knife radiosurgery for brain metastasis of nonsmall cell lung cancer: is there a difference in outcome between morning and afternoon treatment?
, n" D$ J4 M# Q8 u4 M7 T* qRahn DA 3rd, Ray DK, Schlesinger DJ, Steiner L, Sheehan JP, O'Quigley JM, Rich T.2 R% Z/ D4 `; ?- M% ~
SourceDepartment of Radiation Oncology, University of Virginia Health Sciences Center, Charlottesville, Virginia 22908, USA.
# a G4 Q9 {6 m# _1 \, w: a$ [& u) ^) ~8 A+ N5 K% y$ {5 Z M3 @. Y
Abstract
% W3 t3 {* @- D) o# cBACKGROUND: Circadian cell-cycle progression causes fluctuating radiosensitivity in many tissues, which could affect clinical outcomes. The purpose of this study was to determine whether outcomes of single-session gamma knife radiosurgery (GKRS) for metastatic nonsmall cell lung cancer (NSCLC) differ based on treatment time.% Q! f3 k M4 J3 g: Y; H, P( ~
% m3 o. Z& D4 ^2 @" DMETHODS: Fifty-eight patients received GKRS between 10:00 am and 12:30 pm and 39 patients received GKRS between 12:30 pm and 3:00 pm. The mean peripheral dose was 18.6 Gy. The mean tumor size was 7.3 cm³. Magnetic resonance imaging was used to score local control at 3 months. Cause of death (COD) was categorized as central nervous system (CNS)-related or systemic.' T5 _8 G( Y# N2 g! M: Z& ^
0 S3 J' z0 b4 r* o& r bRESULTS: Demographic and disease characteristics of the 2 groups were similar. Local control at 3 months was achieved in 97% (35/36) of patients who underwent GKRS early in the day versus 67% (8/12) of patients who underwent GKRS later in the day (chi-square, P = .014). Early GKRS was associated with better survival (median 9.5 months) than late GKRS (median 5 months) (Kaplan-Meier log-rank test, P = .025). Factors contributing to better survival in a Cox regression model included early treatment time (P = .004) and recursive partition analysis class (P < .001). Cause of death in the early treatment group was CNS-related in 6% (3/47) of patients versus 24% (8/34) of patients in the late treatment group (chi-square test, P = .026)./ L* I, S( m7 n" P
2 m7 w- @( N+ E1 W) ?& N, Y' Q1 x9 ~
CONCLUSIONS: GKRS for metastatic NSCLC had better local control, better survival, and a lower rate of CNS-related cause of death when given earlier in the day versus later in the day. These retrospective data should encourage future study in brain radiosurgery and non-CNS stereotactic body radiotherapy series.7 I2 L5 U1 ]( j. |7 c- A+ `
' k. M3 _6 B$ ^; Y0 X6 v& H |
 根治性放疗结束后,免疫维持两年能不
家父2022年12月份确诊右肺上叶肺鳞癌3A期,纵膈淋巴结转移,一直在复肿治疗,先新辅助
根治性放疗结束后,免疫维持两年能不
家父2022年12月份确诊右肺上叶肺鳞癌3A期,纵膈淋巴结转移,一直在复肿治疗,先新辅助
 这类会“分身术”的肺癌有药了!你变
作者:Tony
目前国内已上市的MET抑制剂有赛沃替尼、卡马替尼、谷美替尼、特泊替尼以及
这类会“分身术”的肺癌有药了!你变
作者:Tony
目前国内已上市的MET抑制剂有赛沃替尼、卡马替尼、谷美替尼、特泊替尼以及
 求助:1a1实体型低分化alk突变复发概
背景:35岁男性,无吸烟史,有熬夜习惯,检查前曾参与新房装修。24年7月底体检第一次
求助:1a1实体型低分化alk突变复发概
背景:35岁男性,无吸烟史,有熬夜习惯,检查前曾参与新房装修。24年7月底体检第一次
 三代伏美换一代特罗凯获益率问题
家父25年2月因肩膀疼痛确诊肺腺癌晚期4B,双肺转,多发骨转,脑转(非典型),
三代伏美换一代特罗凯获益率问题
家父25年2月因肩膀疼痛确诊肺腺癌晚期4B,双肺转,多发骨转,脑转(非典型),
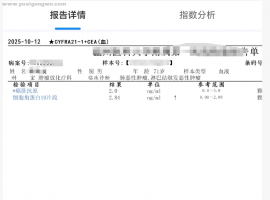 请教下 3a 术后 检查
请教下 3a 术后 检查快两年了, 验血 不是每次都是 肿标 5项吗,我的复查 好像 有时
请教下 3a 术后 检查
请教下 3a 术后 检查快两年了, 验血 不是每次都是 肿标 5项吗,我的复查 好像 有时






 显身卡
显身卡


